Ankle Instability
The word “instability” refers to a situation with abnormal motion.
In order to understand instability, one must first understand stability, or normal motion.
An example: a door opens and closes. This motion is the normal, stable motion for the door. If the hinges became loose and instead of just opening and closing, the door moved also moved up and down, the downward movement with gravity would cause the door to scrape the floor, and the door wouldn’t work right. This abnormal motion is due to instability of the hinges in this example.
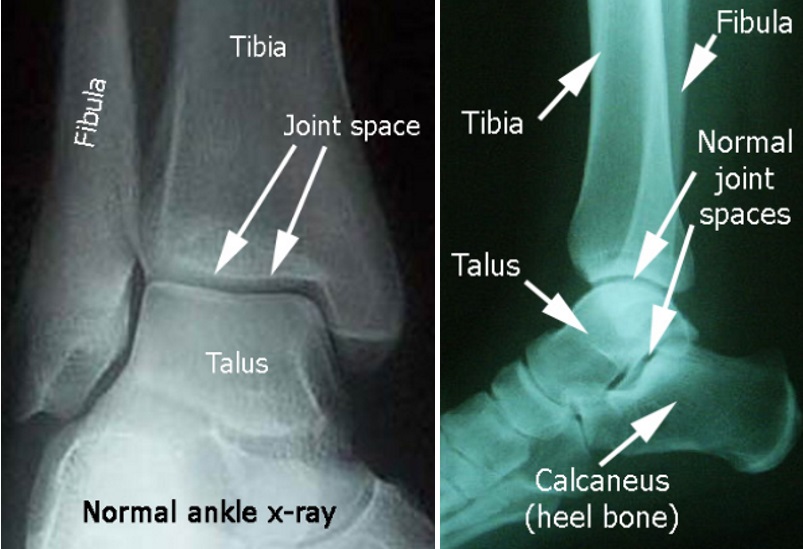
First, here are the normal ankle bones.
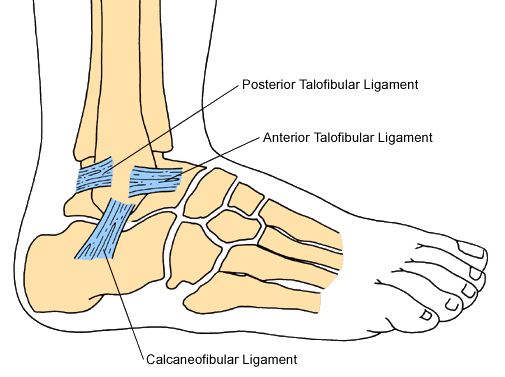
Here is the anatomy of the normal ankle ligaments:
Anterior (towards the front)
Talofibular (connects talus and fibula)
Calcaneofibular (connects talus and fibula)
Posterior (towards back side)
Talofibular (connects talus and fibula)
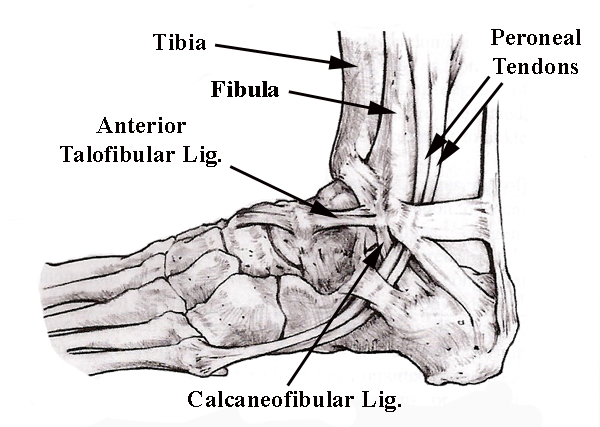
This view shows the same ligaments along with the peroneal tendons, which go behind the fibula, and help to evert the foot (move the ankle towards the little toe side).
Quite often, in cases of instability, these peroneal tendons are working overtime to keep the ankle joint in place. The extra stress on these tendons can lead to peroneal tendonitis.
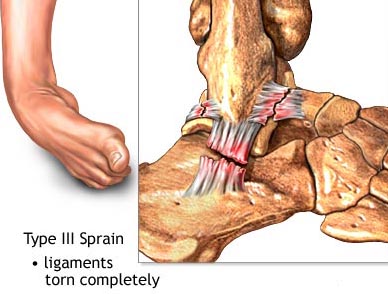
When someone twists their ankle, the first ligaments to tear are the Anterior Talofibular, then the Calcaneofibular, usually in that order. The tear can be partial (grades I or II) or complete (grade III).
The “anterior drawer” test, pictured here, where the foot is pulled forward while stabilizing the leg, is used to check for injuries of the ankle ligaments. An abnormal test is indicated by a feeling of looseness noted by the examiner, with less of this looseness noted on the uninjured side.
Unless this test is done properly, with the patient at least momentarily relaxed, a complete ligament tear can be missed.

Lateral stress X-ray view of ankle here demonstrated a positive “anterior drawer” test, where the foot is pulled forward while stabilizing the leg, The talus moves forward and partially out of the joint indicating ankle instability (abnormal motion).
The views below show X-ray images where the ankle is pulled forward just as the X-ray image is taken. You can see that the talus is partially dislocated anteriorly (towards the front and out of the ankle joint), indicating that the ligaments that normally would hold the talus in place are clearly not doing their job.
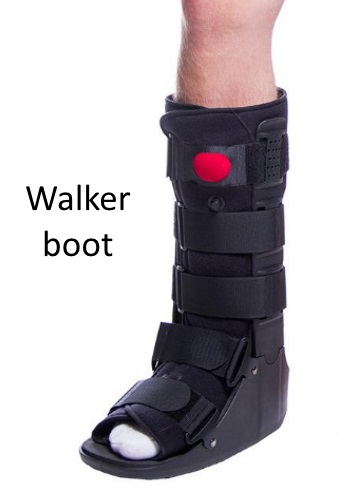
It is important to recognize complete tears in the acute (fresh) setting because often they can be treated with a walker boot very successfully.
When patients are seen soon after their injury, usually four weeks in a walker boot is adequate to avoid need for surgery. However, the boot is to be worn at least 23 hrs a day, including to sleep.
Not wearing boot to sleep is the most common reason why non operative treatment might fail.
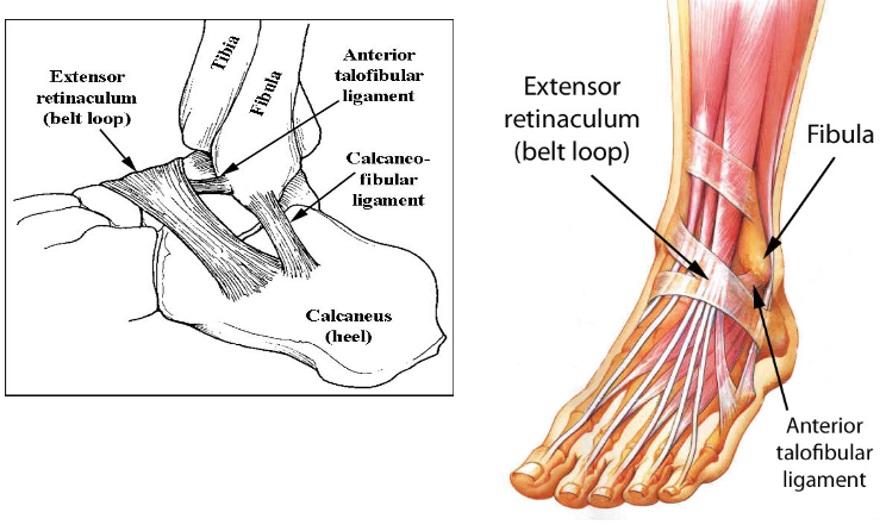
For cases with chronic instability, usually surgery is required for the ankle to regain stability. For considerations regarding stability surgery, the pertinent anatomy is illustrated here.
The extensor retinaculum is like a belt loop, holding the tendons that extend or lift up the toes, down against the surface of the foot and ankle bones, instead of sticking up like the string on a bow (think of bow and arrow).
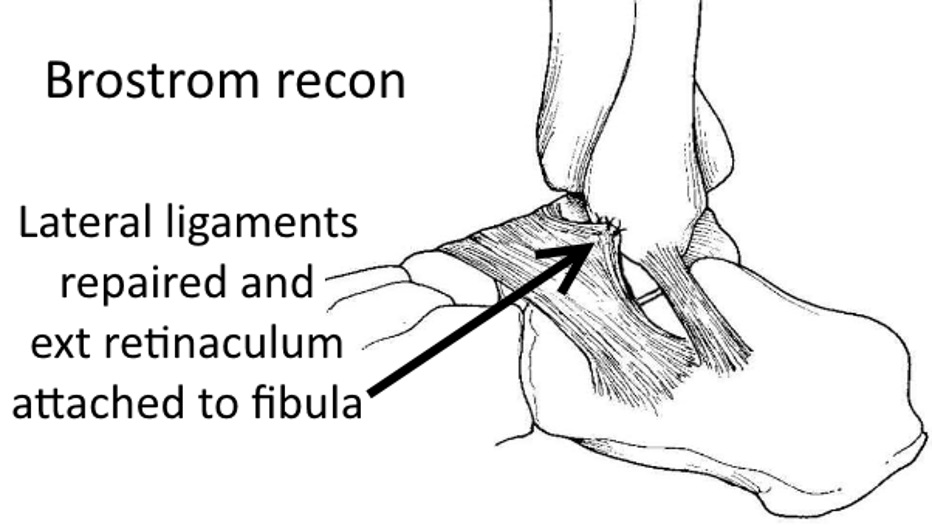
For the Brostrom type repair, the anterior talofibular ligament is reconstructed, either by suturing that ligament together, or reattaching it to the bone, and then the extensor retinaculum is also sutured to the front of the fibula for additional stability.
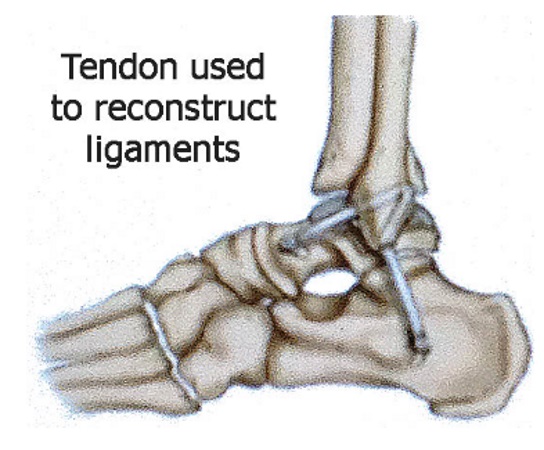
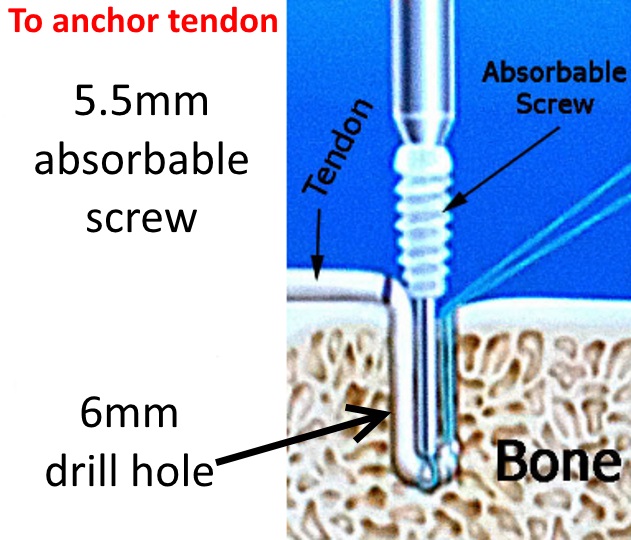
Another technique involves using a tendon from a cadaver, or sometimes harvested from elsewhere in the body, to reconstruct the lateral ankle ligaments, mainly the anterior talofibular, and calcaneofibular ligaments.
The tendon is anchored with a screw that resorbs over time.
In most cases, after surgical reconstruction, the recommendation is that you stay on crutches or use a walker, avoiding full weight on the operated leg, for six weeks after surgery. Since this procedure is elective, it is important to choose a time when you can comply with the limited weightbearing recommendation. Bearing weight too early can jeopardize the repair.
These issues can be discussed more fully at the time of your consultation.